The pupils are tiny, but neurologically they’re loud. With nothing more than a pen torch and a bit of structure, you can gather a surprising amount of information about the brainstem, cranial nerves, and the sympathetic pathway in under a minute.
For GPs, neurologists and students, understanding pupil behaviour is one of the simplest ways to localise disease: is this mainly a sympathetic problem, a parasympathetic problem, or something higher up in the brain?
This article walks through the basics of the light and accommodation pathways, then focuses on three high-yield patterns:
- Horner’s syndrome
- Pupil-involving CN III palsy
- Adie’s tonic pupil
How the Pupils Are Wired (Without the jargon overload)
Two main reflexes matter at the bedside: the light reflex and the accommodation (near) response.
The light reflex – the “wiring to the brainstem”
When light hits the retina, the signal travels:
- Retina → optic nerve (CN II)
- Optic tract → pretectal area in the midbrain
- Pretectal area → both Edinger–Westphal (EW) nuclei
- EW nuclei → via CN III to the ciliary ganglion
- Ciliary ganglion → short ciliary nerves → sphincter pupillae
End result: both pupils constrict when you shine light in one eye (direct + consensual response).NCBI+2NCBI+2
This pathway runs through the dorsal midbrain and midbrain tegmentum, which is why pupil findings are so useful in brainstem pathology.
The accommodation (near) response – the “cortical loop”
The near response uses more cortical input:
- Visual cortex detects a near target
- Signals descend to the supraoculomotor region and EW nuclei
- From EW, parasympathetic fibres again run in CN III to the ciliary ganglion
The result is the classic triad: convergence, accommodation and pupillary constriction. Because this pathway partially bypasses the pretectal area, some disorders affect the light response more than the near response — a key concept in Adie’s pupil and other light–near dissociation states.Department of Neurobiology & Anatomy+1
What “Normal” Looks Like in Real Life
A normal pupil exam is straightforward:
- Pupils are round, equal (or nearly so)
- They constrict briskly to bright light
- They constrict again when the patient focuses on a near object
- In the dark, both pupils dilate symmetrically
When something is wrong, it usually shows up as:
- A size difference (anisocoria)
- An abnormal reaction to light
- An abnormal reaction to near focus
- An abnormal reaction to darkness
The trick is to connect what you see with where the lesion is likely to be.
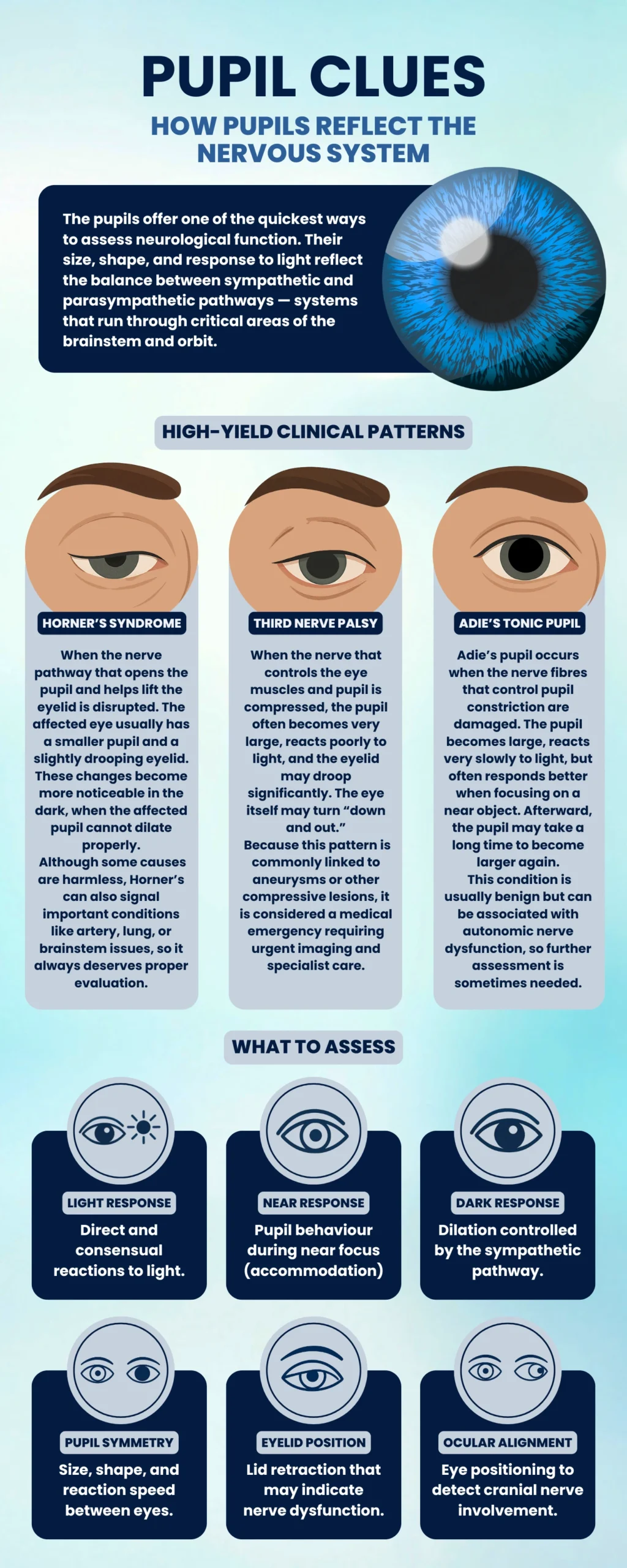
Pattern One: Horner’s Syndrome – A Sympathetic Problem
Key idea: Horner’s is a problem with the sympathetic pathway to the eye.
The sympathetic chain for the pupil runs a long course: from the hypothalamus, down the brainstem, out of the spinal cord, over the lung apex, up the sympathetic chain and along the carotid artery into the orbit. A lesion anywhere on this route can give you Horner’s.
What you see
Classically, Horner’s presents with:
- Miosis – a constricted pupil
- Ptosis – mild upper lid droop
- Anhidrosis – reduced sweating on that side of the face (may be subtle or absent)NCBI+2Physiopedia+2
The affected pupil is small but still reacts to light, and the anisocoria is more obvious in the dark, because the abnormal pupil doesn’t dilate properly. This “dilation lag” is very characteristic.EyeWiki+2EyeWiki+2
Why it matters
Horner’s is a sign, not a diagnosis. Causes range from benign to life-threatening. Well-documented serious causes include:
- Internal carotid artery dissection
- Apical (Pancoast) lung tumours
- Brainstem lesions (stroke, demyelination)
- Neck trauma or surgeryCleveland Clinic+1
For a GP or emergency clinician, the big red flag is new Horner’s with neck pain or headache, where carotid dissection must be ruled out urgently.
Pattern Two: Pupil-Involving CN III Palsy – Think Aneurysm
Key idea: A large, poorly reactive pupil with CN III palsy features suggests compressive pathology until proven otherwise.
The parasympathetic fibres that constrict the pupil travel on the outer surface of the oculomotor nerve. External compression – especially from a posterior communicating (PCom) artery aneurysm – tends to injure these fibres early.NCBI+2EyeWiki+2
What you see
In a typical pupil-involving CN III palsy:
- The pupil is dilated and reacts poorly or not at all to light
- The eyelid is markedly ptotic
- The eye sits “down and out” because the lateral rectus and superior oblique are unopposed
- Diplopia is common
- Pain, especially a sudden severe (“thunderclap”) headache, is a major concernMedscape+1
Why it matters
Multiple neurology and emergency references emphasise that a painful third nerve palsy with a fixed or very sluggish pupil should be treated as a neurosurgical emergency, with rapid imaging to exclude an aneurysm.NCBI+2EyeWiki+2
Ischaemic microvascular CN III palsies (e.g. in diabetes) often spare the pupil, because the central nerve fibres are more affected than the superficial parasympathetic fibres – but this distinction is never an excuse to delay urgent assessment if the clinical picture is worrying.
Pattern Three: Adie’s Tonic Pupil – Benign, But Odd
Key idea: Adie’s is usually a benign post-ganglionic parasympathetic lesion at the ciliary ganglion, often idiopathic.
Adie’s tonic pupil classically affects young women, is often unilateral, and causes a characteristically large pupil with a poor light response but better constriction to near – a “light–near dissociation”.ScienceDirect+3NCBI+3EyeWiki+3
What you see
- One pupil is larger than the other
- The light reaction is weak, slow or absent
- The pupil does constrict when focusing on near objects, but the constriction is slow and “tonic”
- Redilation after near response is also slow
Over time, the affected pupil may actually become smaller (“little old Adie”), but the sluggish, tonic behaviour remains. Adie’s can be associated with reduced reflexes (classically Achilles) in the broader Adie syndrome, but many patients only have ocular findings.NCBI+2Cleveland Clinic+2
Why it matters
Adie’s tonic pupil is usually benign and non-life-threatening, but it’s important to distinguish it from more serious causes of anisocoria. The combination of:
- otherwise normal neurology,
- tonic near response, and
- typical demographic profile
helps clinicians make that call, often confirmed with dilute pilocarpine testing in specialist settings.EyeWiki+1
Using Light, Near and Dark as a Simple Framework
You don’t need a complex algorithm to get a lot out of pupil testing. Many clinical reviews of anisocoria boil it down to three simple questions.RACGP+2EyeWiki+2
What happens in the light?
- If one pupil doesn’t constrict to bright light, think parasympathetic or iris problem:
- CN III palsy
- Adie’s tonic pupil
- Pharmacologic dilation
- Structural iris damage
What happens at near?
- If the light reaction is poor but the near reaction is better (light–near dissociation), Adie’s and other pretectal or post-ganglionic conditions move up the list.
What happens in the dark?
- If anisocoria is worse in the dark and the small pupil fails to dilate, suspect a sympathetic lesion, such as Horner’s syndrome.
- If anisocoria is worse in bright light and the large pupil fails to constrict, suspect parasympathetic dysfunction or pharmacologic mydriasis.
This simple “light–near–dark” mental framework is echoed across neuro-ophthalmology texts and general practice reviews, and works well in busy clinics.RACGP+2OUP Academic+2
Three Short Cases That Tie It Together
Case 1 – The subtle small pupil in the dark
You notice a patient with mild ptosis and a slightly smaller pupil on one side. In a dim room, the asymmetry becomes more obvious; the small pupil is slow to dilate.
That pattern – anisocoria greater in the dark with a small, reactive pupil – fits Horner’s syndrome. If the patient also has neck pain or headache, guidelines and reviews support urgent imaging to exclude carotid dissection.Cleveland Clinic+2WebEye+2
Case 2 – The painful big pupil with a droopy lid
Another patient has a sudden headache, a very dilated pupil, marked ptosis and the eye resting “down and out”. The pupil barely moves to light.
This is the classic picture of a pupil-involving CN III palsy. Because of the strong association with PCom aneurysms, multiple emergency and neurology sources emphasise prompt neuroimaging and urgent neurosurgical input.NCBI+2EyeWiki+2
Case 3 – The odd big pupil in a well young person
A young woman presents with a unilateral, slightly enlarged pupil. She has no pain, no diplopia, no ptosis, and her exam is otherwise normal. The pupil barely responds to light, but when she focuses on a near object it does constrict — slowly — then redilates lazily.
This matches Adie’s tonic pupil, an idiopathic and usually benign post-ganglionic problem described consistently in ophthalmology and neurology literature.ScienceDirect+3NCBI+3EyeWiki+3
Explaining Pupil Findings to Patients
For patients, this can all sound intimidating. A simple explanation that stays faithful to the neuroanatomy is:
“Your pupils are controlled by wiring that runs between your eyes and your brain. When that wiring changes, the pupils can behave differently, which helps us work out which part of the pathway might be affected.”
This way, patients understand why you’re worried about a “funny pupil” even if they feel fine, and why further imaging or referral is necessary.