
In everyday clinical practice, the challenge is not simply performing an eye examination — it is ensuring that clinically significant pathology is not overlooked. Many of the most serious causes of vision loss present subtly, particularly in their early stages, and may easily be dismissed if the clinician is not actively searching for them.
Patients rarely present with textbook descriptions. Instead, they describe vague symptoms such as “slight blurring,” “difficulty with glare,” or “something not quite right.” These seemingly minor complaints often mask underlying pathology that requires careful interpretation and correlation with clinical findings.
A disciplined and structured approach ensures that each anatomical structure is assessed properly, and that important clues are not missed. This article provides a practical, clinically relevant framework that can be applied consistently in real-world practice.
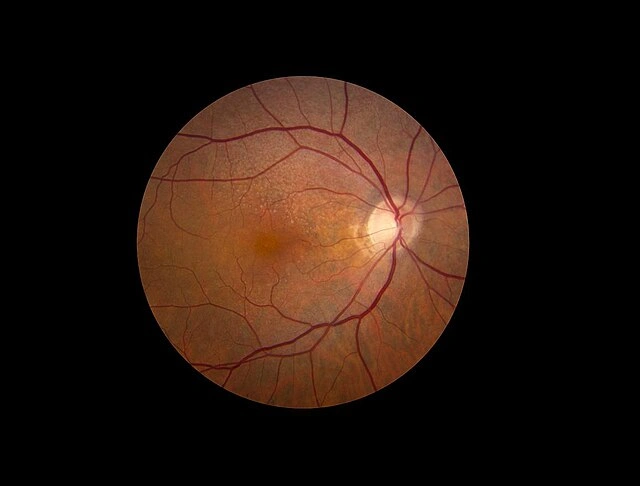
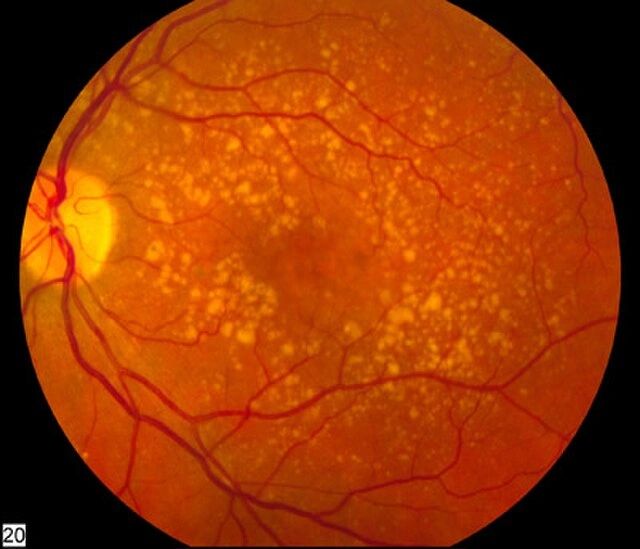
Subtle vs Advanced Retinal Pathology
1. The Clinical Framework: How Experienced Clinicians Think
Before focusing on technique, it is essential to understand how experienced clinicians approach a patient. The examination is not a checklist — it is a process guided by continuous clinical reasoning.
Every patient should be evaluated through three key lenses:
- Structural → Which anatomical structure could be affected?
- Functional → What aspect of vision is impaired?
- Temporal → How quickly has the problem developed?
This triad allows you to begin forming a working diagnosis even before completing the examination.
Clinical Rule
Any unexplained reduction in visual function must be considered pathological until proven otherwise.
2. Visual Acuity: A Diagnostic Tool, Not a Formality
Visual acuity is often treated as a routine measurement, but it is one of the most powerful diagnostic tools available. Its value lies not in the number recorded, but in how that number is interpreted.
A reduction in acuity that improves with pinhole testing typically suggests refractive error or media opacity. In contrast, a reduction that does not improve should immediately raise concern for retinal or optic nerve pathology.
Key Interpretations
- Improves with pinhole → refractive error or cataract
- No improvement → macular or optic nerve pathology
- Asymmetry between eyes → always clinically significant
- Fluctuating vision → tear film instability or corneal disease
A critical habit is to always ask:
“Does the visual acuity match what I am seeing clinically?”
If the answer is no, further investigation is required.
3. Pupillary Assessment: A Rapid Neurological Screen
Pupillary examination is one of the most efficient ways to assess the integrity of the visual pathway, yet it is often underutilised.
The presence of a relative afferent pupillary defect (RAPD) is particularly significant, as it indicates asymmetry in the afferent visual system. This finding may point to optic nerve disease or severe retinal pathology, even when other findings are subtle.
Conditions Associated with RAPD
- Optic neuritis
- Ischemic optic neuropathy
- Advanced glaucoma
- Severe retinal disease
Clinical Insight
Reduced vision + normal anterior segment + RAPD = posterior pathology until proven otherwise.
Because of its diagnostic value, pupillary assessment should never be skipped or rushed.
4. Slit Lamp Biomicroscopy: Precision Over Speed
The slit lamp is arguably the most important instrument in optometric practice, but its effectiveness depends entirely on technique. A quick scan is insufficient — each structure must be examined deliberately.
A systematic approach is essential:
- Begin with low magnification for general overview
- Progress to high magnification for detail
- Use multiple illumination techniques
Essential Illumination Techniques
- Diffuse illumination → general assessment
- Optical section → corneal depth and thickness
- Retroillumination → subtle corneal and lens changes
What to Actively Look For
Cornea
- fine punctate staining
- infiltrates
- dendritic lesions
Anterior Chamber
- cells and flare
- hypopyon
Lens
- posterior subcapsular cataracts
- nuclear sclerosis
Common Pitfall
Many clinicians fail to adjust the beam dynamically. Without changing angle, width, and intensity, subtle pathology is easily missed.
If you are not adjusting the beam, you are not fully examining the eye.
5. Intraocular Pressure: Interpretation in Context
Intraocular pressure (IOP) is an important measurement, but it must always be interpreted within the broader clinical picture.
A key concept is that glaucoma is not simply a pressure problem — it is an optic neuropathy. Many patients with glaucoma have normal pressures, while some with elevated pressures may never develop damage.
Factors Affecting IOP Accuracy
- Corneal thickness
- Patient squeezing
- Poor alignment during measurement
Clinical Integration
IOP should always be interpreted alongside:
- optic nerve appearance
- visual fields
- progression over time
A normal IOP does not rule out glaucoma.
6. Posterior Segment Examination: Where Disease Is Often Missed
The posterior segment is where many vision-threatening conditions are detected, yet it is also where pathology is most frequently overlooked.
A structured approach is critical.
Optic Nerve Assessment
Evaluate carefully:
- cup-to-disc ratio
- symmetry between eyes
- neuroretinal rim
- presence of haemorrhages
Red Flags
- asymmetry >0.2
- rim thinning or notching
- disc haemorrhages
Macular Assessment
The macula requires particular attention, as early disease can be subtle.
Look for:
- drusen
- pigment changes
- subtle oedema
- epiretinal membranes
Clinical Insight
Patients may report:
- “distorted vision”
- “difficulty reading”
These symptoms should never be dismissed.
Peripheral Retina
Often neglected but critically important.
Look for:
- lattice degeneration
- retinal tears
- holes
High-Risk Symptoms
- flashes
- floaters
- curtain-like shadow
These require urgent referral.
7. Visual Field Assessment: Simple but Powerful
Confrontational visual field testing, although basic, can detect significant pathology when performed properly.
Patterns to Recognise
- Hemianopia → neurological pathology
- Arcuate defects → glaucoma
- Central defects → macular disease
Any abnormality should be followed up with formal visual field testing.
8. Pattern Recognition: The Skill That Defines Experience
Over time, clinicians develop the ability to recognise patterns of disease based on symptoms and findings.
Common Clinical Patterns
- Cataract → gradual blur + glare
- Glaucoma → early normal vision + optic nerve changes
- Retinal detachment → flashes + floaters + shadow
- Macular disease → distortion + central vision loss
Pattern recognition improves speed, but must always be supported by thorough examination.
9. High-Risk Presentations You Must Not Miss
Certain presentations require immediate attention and should never be underestimated.
Emergency Red Flags
- Sudden vision loss
- Painful red eye with reduced vision
- New floaters and flashes
- Distorted central vision
These may indicate:
- retinal detachment
- vascular occlusion
- infection
- acute glaucoma
10. Common Clinical Pitfalls
Many missed diagnoses are due to process failures rather than lack of knowledge.
Frequent Mistakes
- rushing the examination
- failing to follow a structured sequence
- over-reliance on imaging
- ignoring subtle findings
A “normal” exam should only be concluded after every structure has been carefully assessed.
11. The Clinical Mindset
Ultimately, the most important tool is the clinician’s mindset. Technical skill must be combined with curiosity, caution, and clinical reasoning.
Ask yourself during every consultation:
- Does this presentation make sense?
- Is anything subtle being missed?
- Is this patient safe without referral?
Final Clinical Principle
If something feels abnormal — even subtly — it should be investigated further.
Conclusion
Examining the eye for pathology requires more than technical ability. It demands a structured approach, attention to detail, and the ability to interpret findings in context.
By combining systematic examination with clinical reasoning and pattern recognition, optometrists can detect disease earlier, refer appropriately, and play a crucial role in preventing vision loss.